
From mortar to cleanroom
There was once a time when the apothecary ground herbs in a mortar and mixed ointments from handwritten prescriptions. When the errand boy ran to the harbour to fetch raw materials from ships docking at the quay, and the quality of medicines depended on the craftsman’s hands and judgement. Control systems were carried by individuals — and differed from one back room to the next.
That was before the industry was established. Before requirements emerged. Before the understanding of connections became clear. The first step on a long journey whose end remains uncertain.
In the mid-nineteenth century, the first recognitions began to take shape. When Ignaz Semmelweis introduced hand washing with chlorinated water in a maternity clinic in 1847, mortality among new mothers fell from nearly 18 % to below 2 %.[1] Yet he was ridiculed. People did not understand that surroundings could cause disease. Sterility was not taken for granted — it was a new idea, and as is often the case, new ideas meet resistance.
Today it seems self-evident. But it shows how great a paradigm shift has taken place. From intuition to sterilisation. From sterilisation to documentation. From documentation to validation.
As the pharmaceutical industry began to take shape at the beginning of the twentieth century, it became clear that experience and tradition were not enough. Production grew — and with it came risks of contamination, error and uncontrolled variation. But it was not civil servants who introduced the first requirements. It was the industry itself. Physicians, pharmacists, engineers and machine builders imposed demands on themselves and their surroundings — not for moral reasons, but to improve production, to grow and expand. It was also they who understood that trust cannot be built at scale without systems and documentation.
And here — in the middle of this development — the vacuum cleaner appeared. Not as a household appliance, but as a tool that over time would have to undergo the same journey as all other equipment: from a cleaning aid to a validatable component in the production environment.

Timeline of the most important regulatory and technical milestones from the formalisation of GMP in the 1960s to EN 17348:2022.
GMP – when cleanliness became a production standard
GMP is not a single rule. It is a mindset: that everything you do must be documentable, controllable and repeatable. That errors cannot simply be corrected after the fact — but must be prevented through procedures, validation and quality management.
Before GMP became a regulatory requirement, many companies began setting their own internal standards for cleanliness and traceability — not for moral reasons, but to ensure growth, credibility and scalability. It was the industry itself that first understood that trust requires systems.
The concept of Good Manufacturing Practice was subsequently formalised in the United States in 1963, following a series of tragic incidents involving contaminated or defective medicines.[2] The WHO followed in the late 1960s, and European GMP came into force in 1989. In 2022, the EU introduced its most comprehensive update to GMP Annex 1 to date — with tightened requirements for particle control, RABS and Contamination Control Strategy in cleanrooms.
GMP is not only about what you produce — but how. Requirements apply to premises, workflows, personnel, equipment and, above all, documentation. And it is precisely here that the vacuum cleaner begins to change its role.
Because if a risk of contamination arises — for instance during powder dosing, granule transfer or spillage of APIs (Active Pharmaceutical Ingredients) — it can no longer be left to the operator to simply “clean up”. Equipment must be used that can document its own function: HEPA filtration, material selection, ease of cleaning, service logs and earthing continuity checks, to name but a few.
A vacuum cleaner for GMP environments is no longer a tool — it is part of the quality management system. It must be validatable on the same terms as all other equipment and must meet the requirements imposed during audits and inspections. This applies not only in pharmaceutical production, but also in food production, laboratories and biotech, where GMP is used as the basis for trust and safety.
GMP is not simply about cleanliness — it is about traceability, responsibility and process control.
A GMP environment must ensure that production takes place in a manner that minimises the risk of errors, contamination and mix-ups. Everything must be documentable, verifiable and validatable.
But GMP must not be confused with technical standardisation. There is no single global GMP standard — only interpretations and implementations: EU-GMP, FDA cGMP, WHO GMP and others. This means two companies can both follow GMP and still choose very different solutions. It is therefore important to understand GMP as a system of principles — not a checklist. And it makes it possible for something to be “GMP-compliant” while still posing a risk from an ATEX or OEB perspective.
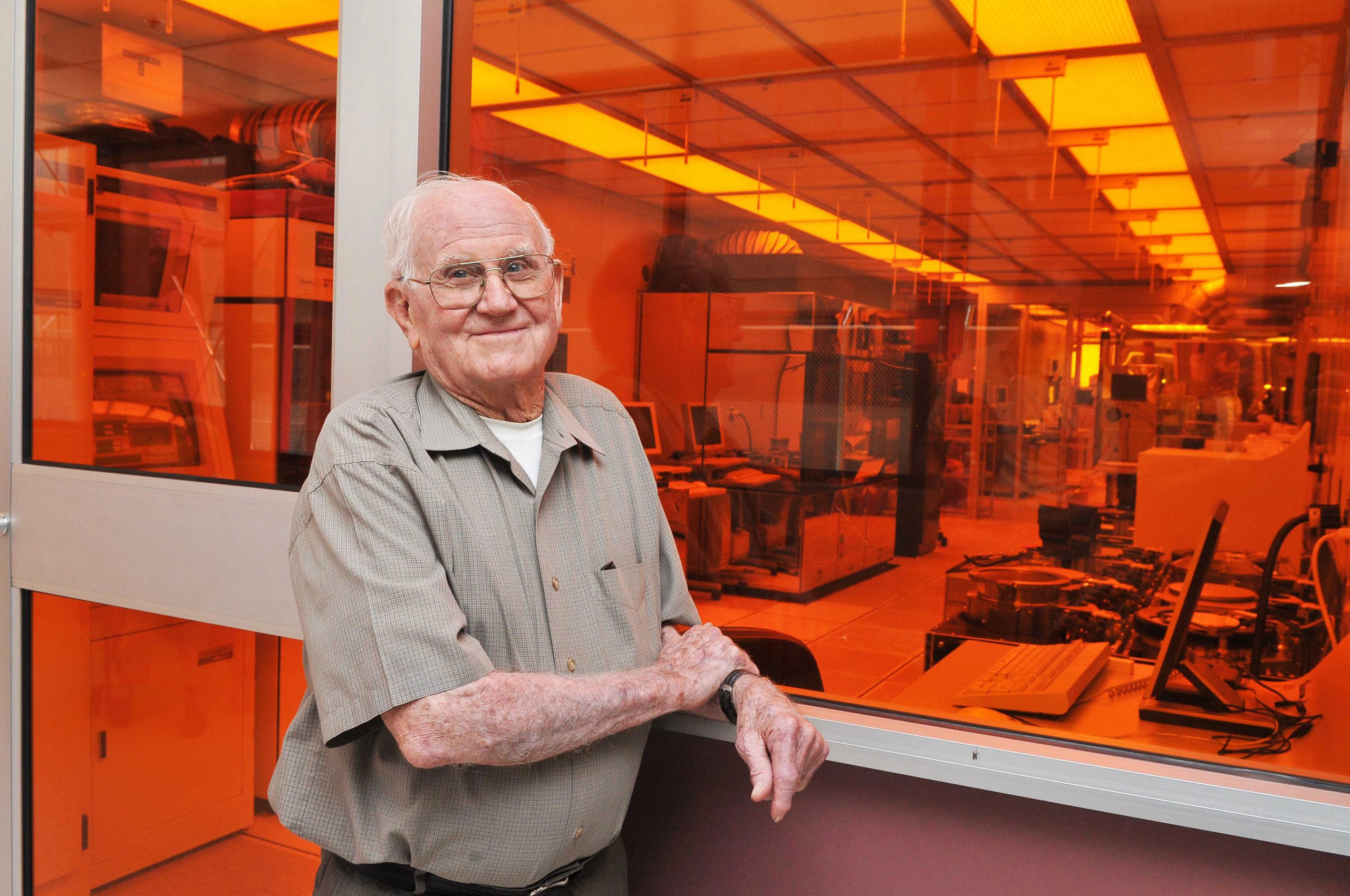
Willis Whitfield in front of his cleanroom at Sandia National Laboratories, USA. Photo: MESA / Sandia National Laboratories.
The birth of the cleanroom
The modern cleanroom was born in 1962, when the physicist Willis Whitfield — working at Sandia National Laboratories in the United States — developed a new system in which air was directed in laminar flow and filtered continuously through HEPA filters.[3] The solution was groundbreaking: it could reduce the number of airborne particles a thousandfold, and it was quickly adopted by the defence industry, the space sector and microelectronics, where even microscopic dust could cause components to fail.
But Whitfield’s work was only the beginning. During the 1970s and 1980s, cleanroom technology spread rapidly to new industries — particularly pharmaceutical production. Local practices developed for zones, ventilation, clothing, surface requirements and particle measurement. The problem was simply that there was no single common standard. The United States used Federal Standard 209E, measuring particles per cubic foot. The United Kingdom used BS 5295. Japan had its own measurement system. And many companies operated under internal rules that could not readily be compared across national borders.
The need for an international standard became clear, particularly as regulatory authorities such as the FDA and EMA began to require documentation of cleanliness and control measures. The cleanroom was no longer merely a technical space — it became a regulatory framework in which measurement data had to be traceable, auditable and usable as documentation.
ISO 14644-1 was therefore published in 1999 as an international compromise and reference point, driven by Technical Committee ISO/TC 209, in which experts from across the world participated. The standard introduced a new measurement principle: a shift to measuring particles per cubic metre of air, with a logarithmic classification scale and defined threshold values for each ISO class.[4] For the first time, common requirements could be established for both measurement equipment and sampling methods. In 2015 the standard was revised with tightened requirements for measurement uncertainty and data analysis.
Today, the cleanroom is not merely a technology, but an interplay of architecture, airflows, material selection and process control. In pharma, cleanrooms play a central role — particularly when GMP, OEB and ATEX requirements converge in the same environment.
For a technician it is natural to speak of particle limits and measurement uncertainty. But for the operator inside the room, reality is often different: one wrongly lifted lid, one unprotected hand movement, and tomorrow’s measurement falls outside the limit — without anyone knowing why. ISO 14644 makes particles measurable. But it does not always make the cause visible.
ISO 14644-1 defines the classification of air cleanliness in cleanrooms based on particle concentration — not on the hazardousness of the particles.
It measures how many particles above a given size are permitted per cubic metre of air. A classification such as ISO 5 or ISO 8 indicates how controlled the environment must be — the lower the number, the cleaner the air.
This sounds precise, but the standard says nothing about the content, origin or consequences of the particles. It measures quantity only — not hazard. An area can therefore comply with ISO 14644 and still be contaminated with, for example, explosive or health-hazardous particles. ISO 14644 is therefore not sufficient on its own when working with substances that also have ATEX, GMP or OEB relevance.
OEB – controlling the invisible

In most industries, it is the dust that poses a hazard to the surroundings. But in pharma, biotech and laboratories, the situation is often reversed: the surroundings are hazardous to the dust — that is, to the product, or more precisely, to what the dust contains. An active pharmaceutical ingredient (API) loses its purity if contaminated by other substances — and it can be directly harmful to those who handle it.
The industry therefore developed a system for classifying hazardous substances according to the level of protection their handling environment must provide. Occupational Exposure Band — abbreviated OEB — became the most widely used classification system. It is not a law, nor a formal standard, but a method for assessing risks and making decisions about how to protect both product and operator. The system emerged in the late 1980s and early 1990s, driven by the British pharmaceutical industry and subsequently developed further by ISPE.[5]
When working with substances at OEB 4 or 5, we are dealing with materials where even minute quantities in the air can pose a health risk. The exposure limit — the maximum permissible amount — often lies as low as micrograms per cubic metre of air. This is equivalent to a single grain of sugar distributed throughout a large room. In other words: it takes almost nothing before exposure becomes too high.
It is therefore not sufficient for a room to be well-ventilated or to appear clean at a glance. Every movement, every surface and every dust particle counts when working with substances designed to affect biological processes in extremely small doses.
And again it became clear that even cleaning equipment must be designed with care. A misplaced vacuum cleaner can function as a source of contamination, not as a solution — if, for instance, it sheds fibres, creates air turbulence, removes air that must then be replaced, introduces air through automatic filter-cleaning systems that cause overpressure, or if it is impossible to document what has been collected. Specific vacuum cleaners were therefore developed for OEB areas: often with closed filter changes, encapsulation of motor components, GMP documentation and the possibility of inerting the collected material.
OEB is at the time of writing not a unified global standard, but a number of actors — including ISPE and national authorities — recognise OEB principles as good practice in the assessment of exposure risks. The EMA’s Annex 1 does not refer to them directly, but in practice builds on the same thinking. It remains largely the responsibility of individual companies to define the limits, conduct the risk assessment and implement the necessary protective measures.
Until that changes, we must work with what we know: that invisible particles are often the most hazardous — and that documentable control of the process environment is not a choice, but a necessity.
OEB stands for Occupational Exposure Band — a method for classifying substances according to how hazardous they are to inhale or absorb through the skin.
The system is used primarily in the pharmaceutical industry, where potent active substances are handled that can have serious health effects even at very low exposures. OEB is not legislation, but an industry model developed by pharmaceutical companies to manage risk. It functions like a funnel: the higher the OEB class, the more stringent the requirements for technical and organisational barriers — such as isolators, negative pressure, closed filter changes and appropriate PPE.
But OEB alone is not sufficient. An OEB 5 substance may also pose an explosion risk (ATEX), or may be so potent that even an ISO 14644-classified measurement fails to reveal the real danger — because the standard counts particles, not assesses toxicity. OEB must therefore always be evaluated in combination with other risks.
Do you work with OEB-classified substances?
We provide advisory on equipment selection for OEB facilities based on your specific environment, your substances and your internal requirements — not from a standard catalogue. Contact us for a no-obligation conversation or explore our OEB products.
ATEX – when air itself becomes a hazard zone

In work with OEB-classified substances, the focus is on protecting people from the substance. But in some situations the picture is reversed — or becomes twofold: here it is not only the substance that must be kept away from the body. It is the body and its surroundings that must be protected from the substance’s effect in the air. Because when air mixes with fine combustible dust, even an invisible cloud can become an ignitable atmosphere. This is not merely a health risk. It is an explosion hazard.
ATEX begins where the air itself becomes the hazardous ingredient.
The term derives from the French Atmosphères Explosibles and was consolidated into EU legislation in 1994 (Directive 94/9/EC), later updated in 2014 (Directive 2014/34/EU).[6] But the concept is older than the legislation. It traces back to the mines and coal dust explosions — the fundamental question: how do we protect people and their surroundings when even the air can ignite?
The problem was known long before it was regulated. In mines, a single spark could collapse entire tunnels. The risk later moved into mills, bakeries, aluminium plants and pharmaceutical production. Wherever fine, dry material was moved, poured, crushed or packed, the air could become explosive — and it was not necessarily open flame that ignited the mixture. It could be friction, static electricity, an overheated motor, a person wearing synthetic clothing.
ATEX standards did not emerge as a narrow technical specialism, but as a cross-cutting safety framework — a way of incorporating everything from buildings and equipment to workflows and ventilation systems into a unified risk assessment. And there — in the middle of this development — the vacuum cleaner came back into play.
Because if dust must be removed, sweeping it away is not the answer. It must be vacuumed up — quickly and efficiently. But also safely. Without the vacuum cleaner itself becoming a source of sparks or overpressure. The ATEX vacuum cleaner therefore required a thorough redesign: with conductive materials, equipotential bonding, defined electrical resistance, low-heat motors — and above all: certification from an independent notified body.
And as with so much else in industry, the development began with one question — and led to many more. While a vacuum cleaner could initially be ATEX-certified as an electrical unit, it remained unclear how the entire collection system should be assessed: what happened inside the container, inside the filter, within the airflow? Was it still safe once the combustible dust had been collected?
It was not until the standard EN 17348:2022 that a genuine answer emerged. Here it was defined how a vacuum cleaner for combustible dust must be constructed, tested and documented. The standard’s focus was not only on resistance to explosion — but also filtration, airflow, tightness, material selection and the ability to ensure that the collected material does not itself create an internal ATEX zone.[7]
It was a milestone. For the first time, a vacuum cleaner could be assessed not merely as a machine — but as a complete solution within an explosive environment. EN 17348 thus became a kind of technical bridge between ATEX, GMP and OEB.
EN 17348 is the European standard for the filtration of combustible dust in vacuum cleaners and dust collectors.
It specifies how equipment must be constructed, tested and marked if it is to be used in areas with explosion risk (ATEX Zone 20 and 22). The standard applies only to equipment used for vacuuming or handling dust — not liquids or gases. EN 17348 sets requirements for:
- Filter placement and integrity
- Container construction (Zone 20 internally)
- Documentation of filtration efficiency
- Tightness testing and maintenance
Many vacuum cleaners are marketed as “ATEX” without complying with this standard. It is therefore important to look for correct marking and technical documentation — not merely promotional claims.
A responsibility that reaches far beyond the laboratory
There is scarcely an industry in which regulation, responsibility and documentation carry more weight than in the pharmaceutical and biotechnology sector. This is not only about drug manufacturing or high-end research. It is about the entire ecosystem of people, equipment, materials and infrastructure that works in — or around — the environments where errors must not occur.
For every laboratory measuring at the nanogram level. For every cleanroom-zoned production line where a single dust particle can mean the difference between an approved and a rejected batch. For every QA specialist signing off on a batch, or the EHS department involved throughout the entire selection process before start-up. There is a chain of subcontractors, service partners, procurement managers, engineers and installation technicians who must all understand and comply with the same standards.
It is not implausible that several million people globally work in — or in close proximity to — these environments. Everything from medicotechnical packaging production in Poland, API synthesis in Switzerland, research in Denmark, audits in Germany and specialised transport in the Netherlands is part of this reality. Without them — no product, no treatment, no trust.
Our journey with the industry — from noise levels to regulatory requirements

Particulair became part of this ecosystem in 1991 — not with ambitions of supplying solutions to the world’s largest companies, but because a production department at Novo Nordisk asked for our help. They wanted a small, compact vacuum cleaner that was quieter than the older Nilfisk models. Noise level and functionality were the priorities — and if it had a HEPA filter and was easy to handle, that was more than sufficient.
At that time, validation, airborne risks and particle levels were a somewhat abstract concept when talking about vacuum cleaners. But the requirements changed, and we changed with them.
Today we advise some of the largest actors in pharma, biotech and high-end laboratories — not because we have the largest organisation, but because we understand the complexity, follow the standards closely and combine knowledge with experience. When we step into a production environment, we do not simply see hoses and machines — we see airflow pathways, flow directions, risk analyses and validation requirements. We ask questions the customer understands — and we collaborate with leading manufacturers to supply equipment that not only meets current requirements, but is prepared for the ones to come.
Not everything is possible. There are physical laws governing volume, flow and filtration that neither we nor the industry can change. But we can listen. Understand. Assess. And offer what makes technical and regulatory sense — even when that requires compromise.
Can we help you navigate the requirements?
We offer advisory on vacuum technology in clinical environments — from equipment selection to assistance with validation and documentation. Read about our advisory services or browse our product range.
When you understand the whole picture, you choose differently
It is tempting to believe we have reached our destination. That everything is now regulated, standardised and documented. We have GMP for quality, ISO 14644 for particles, OEB for exposure, ATEX for explosion hazards and EN 17348 for filtration. But the truth is that every time we identify a new area of risk, we run the risk of forgetting the previous one. And in the effort to meet one requirement, we easily overlook another.
Because people cannot hold everything in mind at once. When one person becomes responsible for GMP and another for ATEX, a blind spot emerges. When OEB requirements meet cleanroom requirements, compromises can arise that no one has thought through — simply because the task is too complex for any one person to grasp all the consequences.
Silos do not arise from ill will. They arise because we have specialised — and because we have elevated standards into truths. But what is true within one standard may be insufficient within another. A vacuum cleaner can be approved for ATEX Zone 22 and simultaneously pose a contamination risk in a GMP area. It may have a closed filter change in accordance with OEB, but still lack earthing continuity in accordance with EN 17348. It may have a HEPA filter but emit particles that go undetected in an ISO 14644 measurement.
Standards help us do the right thing — but they do not tell us what matters. That requires judgement, collaboration and understanding. It requires someone who knows the systems — and someone who knows the connections between them.
Because it is not always the most advanced equipment that makes the difference. It is the person who understands the whole picture who chooses correctly.
Epilogue: The next step

It is many years since the apothecary stood bent over a mortar, grinding herbs with care and hope. Treatments were then created from intuition, experience and a measure of good fortune — and if something failed, it was met with new attempts, not with procedures and traceability requirements.
Yet something keeps repeating itself. Because historically we have almost always thought of the product — the medicine — before the surroundings. First we developed the active substance, and then we built the system around it. First the effect — then the validation. That, broadly speaking, is how the mortar became the cleanroom.
Now we may be facing yet another repetition. Several of the world’s leading pharmaceutical companies are today working with advanced AI and supercomputers. These systems can predict disease patterns, design proteins and simulate biological reactions long before anyone has touched a test tube. They can model treatments at the individual level and calculate how new compounds will behave before the trial phase has even begun. And it is only after that knowledge has been obtained that the need arises to design a production process — and the environment required to support it.
But with supercomputers and artificial intelligence, we gain the opportunity to break the traditional pattern. Perhaps this means that in future we will develop medicines, cleanrooms and production equipment in parallel. A platform that brings together standards, experience and technical requirements across disciplines — and advises: if your finished product requires production facilities at OEB 5 and ISO Class A, you must account for the following cleaning procedure, fire protection, ventilation, surface design, ATEX zones and so on. The company receives a complete plan, ready to be acted upon the moment the compound is approved for production.
The next step is therefore not a new rule, standard or law. It is a new tool. A digital decision-making capability that does not merely tick boxes — but creates connections. A place where questions can be asked that would otherwise require five experts and a joint meeting. Where complexity is not suppressed, but translated. Into understanding. Into action. Into solutions.
Because even when the batch is validated and the documentation is in order, we must never forget that it is ultimately about a human being who needs to get better.
- EMA. EudraLex Volume 4 — EU GMP Guidelines, including Annex 1 (2022). health.ec.europa.eu
- European Commission. ATEX Directive 2014/34/EU. single-market-economy.ec.europa.eu
- ISO 14644-1:2015 — Cleanrooms and associated controlled environments — Part 1: Classification of air cleanliness by particle concentration. iso.org
- EN 17348:2022 — Combustible dust — Vacuum cleaners and dust collectors for use in potentially explosive atmospheres. en-standard.eu
- Sandia National Laboratories. Willis Whitfield — A Simple Man with a Simple Solution that Changed the World (2024). sandia.gov
- WHO: who.int
- EMA: ema.europa.eu
- ISPE: ispe.org
- FDA: fda.gov
- ISO/TC 209: iso.org/committee/51014